

Collagen supplements may provide amino acids and biologically active peptides, but they do not directly rebuild skin, joints, tendons or bone on command. Collagen synthesis depends on digestion, absorption, tissue demand, mechanical loading, adequate cofactors, and product quality. The body still decides where the materials go.
You’ve seen the tub.
Maybe it was sitting beside the protein powders at the chemist. Maybe it was in someone’s smoothie on Instagram, because apparently no supplement is real until it’s been photographed next to a beige kitchen bench. Maybe a patient mentioned it in clinic and asked the question that always sounds simple until youtry to answer it properly.
“Do you think collagen actually works?”
In Warrnambool, I’m hearing this more often.
Not from people chasing miracles. Usually from sensible people who are trying to make a reasonable decision. Their knee is getting cranky. Their skin feels different than it did ten years ago. Their tendon has been grumbling through gym, gardening, running, netball, work, or that brave little return to Pilates after six months of “I’ll start next week.”
They’re not silly.
They’re just standing in front of a shelf full of promises.
And collagen is a tricky one, because it is not complete nonsense. That would be easier. We could all point, laugh politely, and move on.
But collagen is also not magic repair powder.
The best way to understand collagen supplements is this: they may provide building materials, and possibly some biological signals, but they do not decide what your body builds. That decision belongs to your tissues.
Your cells.
Your loading habits.
Your nutrition.
Your recovery.
Your biology.
That’s what this guide is about.
We’ll walk through what collagen actually is, what happens when you swallow it, why “absorbed” does not mean “sent straight to your sore knee,” and why movement matters if you’re trying to influence tendon, bone, joint or connective tissue adaptation.
We’ll also look at what I’d want to see before giving a collagen product even a cautious nod.
Not a miracle.
Not a scam.
Something more interesting.
A maybe.
📌 KEY TAKEAWAYS:
- Collagen supplements do not get installed directly into your skin, joints, tendons or bones.
- Hydrolysed collagen peptides may be absorbed as amino acids and small peptides, some of which may be biologically active.
- Collagen synthesis depends on local tissue demand, mechanical loading, adequate protein, vitamin C, iron, copper, zinc, and broader health.
- Product quality matters. “Collagen” on a label does not mean it matches the product used in clinical research.
- The strongest practical argument is collagen as an adjunct to good nutrition and appropriate loading, not a standalone fix.
Collagen Is Not Just a Beauty Word
Collagen is the main structural protein family in the extracellular matrix. It gives structure, tensile strength and organisation to tissues including skin, tendon, ligament, bone, cartilage, blood vessels and fascia. There are many types of collagen, but type I collagen is especially important in skin, tendon, ligament and bone (Gelse et al., 2003; Amirrah et al., 2022).
That matters because collagen is not one thing doing one job.
Skin does not use collagen the same way tendon does. Cartilage is not tendon with a different postcode.
Bone is not just collagen plus calcium sprinkled on top like parmesan. Each tissue has its own cells, rules, loading environment and repair demands. This is where supplement marketing gets a bit slippery.
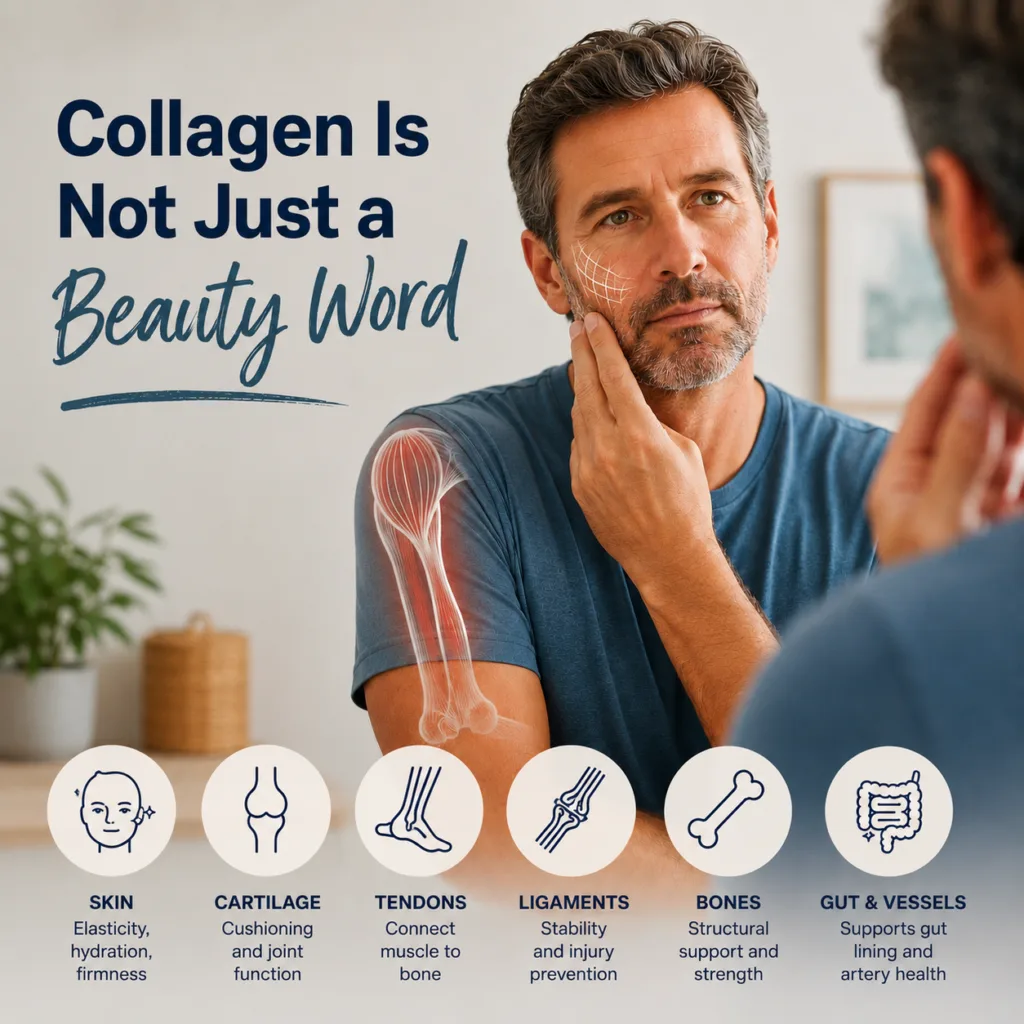
A product can truthfully say collagen is found in skin, joints, tendons and bones. That part is fine.
The leap is when it implies that eating collagen sends collagen directly to those tissues like a courier with
GPS coordinates and a tiny clipboard.
That is not how biology works.
Collagen is built by cells. Fibroblasts, tenocytes, chondrocytes, osteoblasts and other connective tissue cells respond to their local environment.
They decide what gets made, what gets remodelled, and what gets ignored. The supplement does not run the job site. It may deliver materials. That’s different.
What Happens When You Swallow Collagen?
Here’s the important bit.
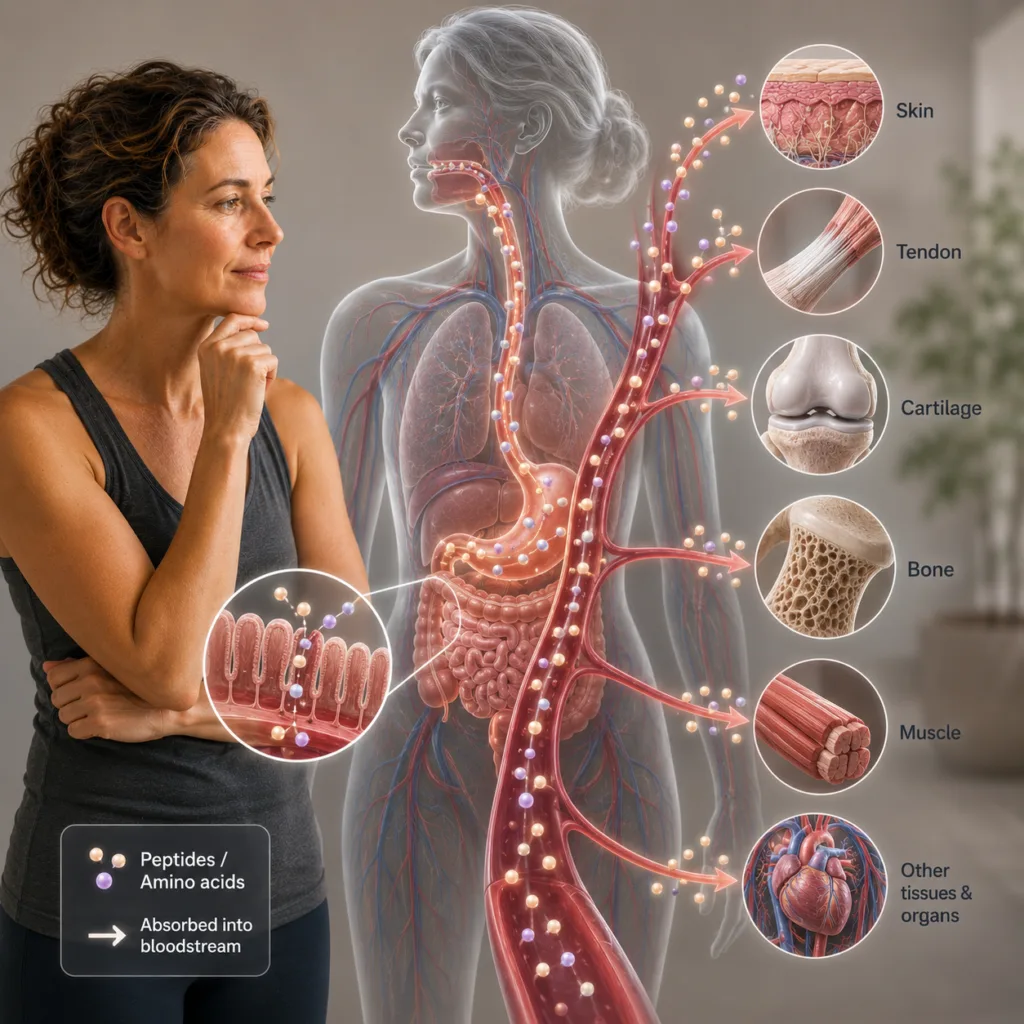
Native collagen is a large triple-helical protein. You do not absorb it intact in any meaningful way. Your digestive system breaks it down.
Most supplements are therefore sold as hydrolysed collagen, collagen peptides, or collagen hydrolysate.
Hydrolysis breaks collagen into smaller peptides. Reviews describe hydrolysed collagen as a mixture of low 3molecular weight peptides, often around 3–6 kDa, produced through processing methods such as enzymatic hydrolysis (León-López et al., 2019).
So the basic pathway looks like this:
collagen supplement → digestion → amino acids + small peptides → absorption →circulation → substrate pool and possible signalling → local tissue response
That is the clean model.
Not glamorous.
Useful.

Some of those smaller peptides, especially hydroxyproline-containing dipeptides and tripeptides, appear to survive digestion and show up in the blood after ingestion. Human bioavailability research has found collagen-derived amino acids and di/tripeptides in circulation after collagen hydrolysate intake, with source and molecular weight influencing peptide profiles (Virgilio et al., 2024).
This is why the old dismissal of collagen as “it just gets broken down, so it’s useless” is too blunt.
Yes, it gets broken down.
But some of the breakdown products may still matter.
The body may use collagen-derived amino acids as substrate. Some absorbed peptides may also act as biological signals, influencing fibroblast behaviour or extracellular matrix metabolism in experimental settings (Sato et al., 2020).
That does not mean they rebuild your skin, tendon or cartilage on command.
It means they may not be inert.
That is a smaller claim.
Absorbed Does Not Mean Directed
This is the bit patients need to understand, because it cuts through a lot of the confusion.
If a collagen peptide appears in the blood, that tells us something useful. It tells us the supplement has been digested and some collagen-derived components have entered circulation.
But it does not tell us where they go.
It does not tell us your body has chosen your sore Achilles tendon.
It does not tell us your knee cartilage is being rebuilt.
It does not tell us your skin has received a special delivery and is now planning a glow-up.
Absorption is not direction.
Your body has an amino acid pool. It has tissues with different demands. It has cells responding to local signals. It has limited resources and priorities. Collagen synthesis happens when local cells are stimulated to make collagen and have enough substrate and cofactors to do the job.
That’s the line I keep coming back to:
Local cells decide, under systemic constraints.
Skin fibroblasts respond to skin conditions. Tenocytes respond to tendon loading. Osteoblasts and osteocytes respond to bone strain, hormones and mineral status. Chondrocytes respond to the cartilage environment, mechanical compression and inflammation.
The supplement does not overrule that.
It joins the conversation.
This is where the naturopathic and osteopathic viewpoints meet nicely.
From the nutritional side, we care about substrate, digestion, absorption, cofactors and tissue repair capacity. From the osteopathic side, we care about load, movement, tissue behaviour and whether the body is receiving a clear reason to adapt.
You need both sides of the conversation.
Because building materials without workers are just a pile of timber in the rain.
The Cofactor Problem: Collagen Needs Tools
Making collagen is not just a matter of having amino acids available.
The body needs tools.
Vitamin C is one of the big ones. It is required for prolyl hydroxylase and lysyl hydroxylase activity, enzymes involved in collagen biosynthesis and stability (Pinnell, 1985). That is why vitamin C deficiency causes connective tissue problems: poor wound healing, fragile vessels, bleeding gums and impaired collagen integrity.
Iron and oxygen are also involved in hydroxylase enzyme function. Copper is important for lysyl oxidase activity, which helps cross-link collagen and elastin. Zinc plays broader roles in protein synthesis, cellfunction, wound healing and tissue repair.
So if someone takes collagen peptides but has poor overall nutrition, low protein intake, low vitamin C intake, poor energy availability, poor sleep, or high stress load, the supplement may be trying to work in a messy system.

This is where I become deeply boring and annoyingly correct.
The basics matter.
- Adequate protein.
- Enough energy.
- Fruit and vegetables.
- Vitamin C.
- Mineral status.
- Sleep.
- Movement.
- Recovery.
Not exciting.
Still true.
A collagen supplement does not need to contain every cofactor in the same scoop. The body can draw from dietary intake and existing stores. But if those stores are low or the person’s diet is poor, collagen peptides alone may not be enough to move the needle.
The building materials arrive. But the tools are missing.
Why Loading Changes the Conversation
This is where the osteopathic view becomes important.
Tendon, ligament and bone are not passive tissues waiting around for supplements to rescue them. They respond to load.
Mechanical loading is biochemical information.
In tendon, mechanical forces influence tenocyte behaviour, collagen turnover and extracellular matrix organisation. Reviews on tendon mechanotransduction describe loading as central to tendon homeostasis, adaptation and repair (Nakamichi et al., 2024). Earlier work also links tendon collagen synthesis and degradation to both acute and chronic loading (Magnusson et al., 2010).
That means a tendon does not simply ask, “Did collagen arrive?”
It asks, “Is there a reason to remodel?”
That reason often comes from mechanical stimulus.
Appropriate loading tells the tissue there is a job to do. Too much load can irritate it. Too little load can leave it under-stimulated. The sweet spot is rarely dramatic. It is usually progressive, boring, patient-specific, and annoyingly effective over time.
If you’re building collagen into a bigger plan
The Centenarian Decathlon: A Blueprint for Lifelong Strength & Resilience →
Why training for what you want to do at 80 changes what you do today.
The same broad principle applies to bone.
Bone cells respond to mechanical strain. Osteocytes act as key mechanosensors, converting loading into biochemical signals that influence bone formation and resorption pathways (Li et al., 2021). Bone adaptation involves osteoblasts, osteoclasts, osteocytes, mineral status, hormones, vitamin D, calcium, inflammation, and mechanical load.
Again, collagen may provide substrate.
But loading provides the instruction.
That is why collagen plus no movement is a weaker argument than collagen plus appropriate loading, adequate nutrition and a tissue that is actually being asked to adapt.
It is not about smashing the body.
It is about giving the right signal.
What Does the Research Actually Say?
The research is promising in places, but it is not clean enough for big shiny claims.
Skin
There is evidence that hydrolysed collagen supplementation may improve skin hydration and elasticity in some trials. A 2023 systematic review and meta-analysis of 26 randomised controlled trials reported. improvements in skin hydration and elasticity compared with placebo (Pu et al., 2023).
That sounds useful.
But then comes the bucket of cold water, which every good evidence conversation needs.
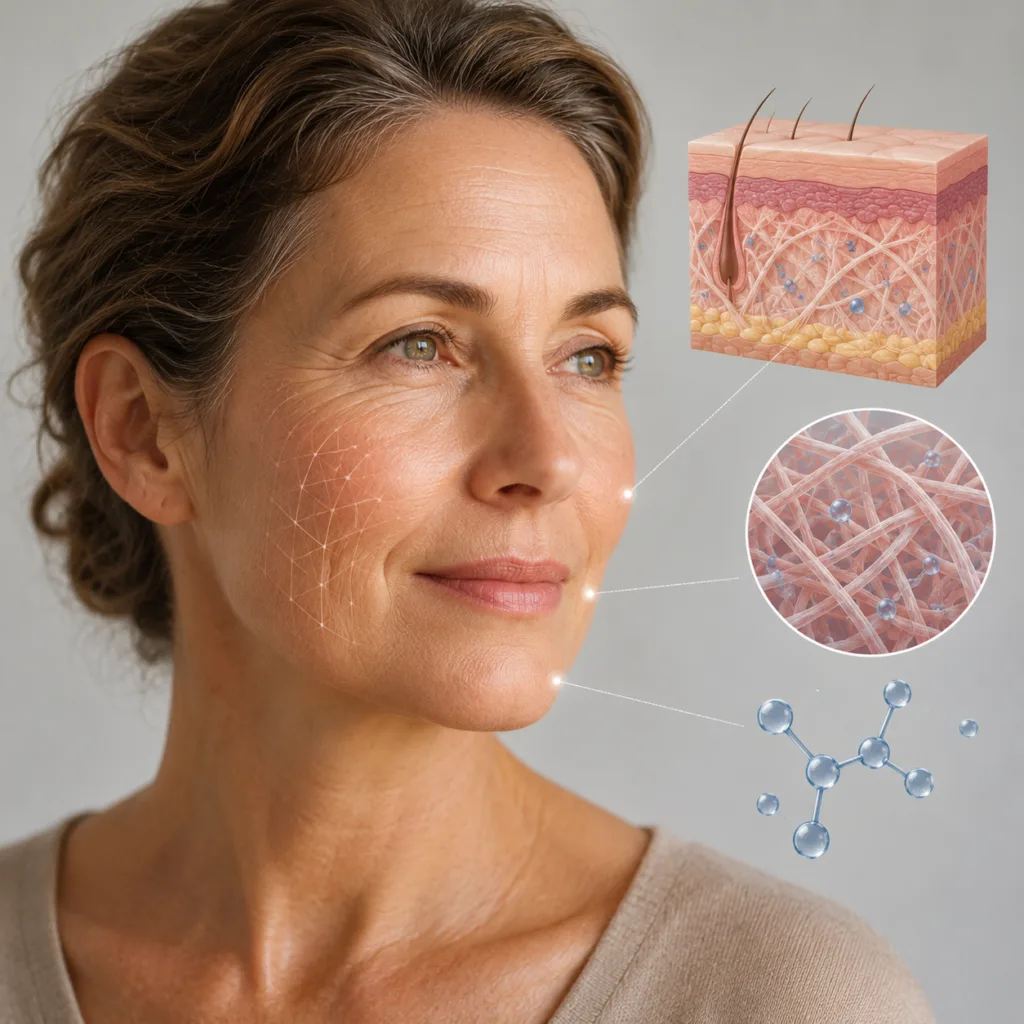
A 2025 meta-analysis found collagen supplements improved skin hydration, elasticity and wrinkles overall, but when the authors separated studies by funding source, studies without pharmaceutical company funding did not show significant benefit, while industry-funded studies did (Myung & Park, 2025).
That does not prove collagen does nothing.
But it does tell us to be careful.
“Skin glow” is not a mechanism. It is marketing language wearing a lab coat.
Joints and osteoarthritis
For knee osteoarthritis, a 2023 meta-analysis of randomised controlled trials found collagen peptides were associated with significant pain relief compared with placebo, but the authors also noted limitations and the need for better trials (Lin et al., 2023).
That makes collagen a reasonable discussion point for some people.
But not a replacement for strength work, load management, medical care, weight management where relevant, sleep, general diet, or the other boring levers that actually shape joint health.
A supplement may reduce symptoms for some people.
It does not restore a joint to factory settings.
Tendons, ligaments and training
This is the area I find most biologically interesting.
A well-known study found that vitamin C-enriched gelatin taken before intermittent exercise increased markers associated with collagen synthesis, with the authors suggesting gelatin combined with exercise may support tissue repair and injury prevention contexts (Shaw et al., 2017).
A 2024 systematic review and meta-analysis looked at collagen peptide supplementation combined with physical training and found promising, though low-to-moderate certainty, evidence for improvements in fat- free mass, tendon morphology, muscle mass, maximal strength and some recovery measures (Bischof et al., 2024).

That is not a green light for hype.
It is a useful signal.
The most defensible position is that collagen may be more plausible when paired with loading than when taken passively.
Materials plus job order.
That’s the model.
The Product Problem: Not All Collagen Is the Same
This is where things get messy.
“Collagen” is not one standardised intervention. A product might be bovine, marine, porcine or chicken-derived. It might come from skin, hide, bone, cartilage, scales or other connective tissue. It might be native collagen, gelatin, hydrolysed collagen, or a blend. It may have different molecular weights, peptide profiles, doses, additives, flavours, sweeteners, quality controls and contaminant risks.
The label might say collagen.
That does not tell you enough.
Hydrolysed collagen products vary depending on source material, extraction method, hydrolysis process and molecular weight distribution (León-López et al., 2019; Virgilio et al., 2024). Reviews on collagen type I biomaterials also emphasise the complexity of collagen source, processing, isolation and purification (Amirrah et al., 2022).
This matters because a study using one specific collagen hydrolysate at a specific dose for a specific population over a specific time frame does not validate every tub on the shelf.
That is the category trap.
Patients say, “I’m taking collagen.”
But clinically, that is like saying, “I’m doing exercise.”
Good start.
What kind?
How much?
How often?
For what goal?
What else is happening?
Without those details, we are mostly guessing.
And supplement marketing loves it when we guess.
📌 Collagen supplements may support the system,
but they do not direct the system.
A Simple Collagen Product Scorecard
I would not choose a collagen product based on the loudest claim on the front of the tub.
I’d look at the quiet details on the back.
1. Is it hydrolysed collagen or collagen peptides?
For absorption, hydrolysed collagen peptides are generally the more plausible form. Native collagen is not absorbed intact in a meaningful way.

Green flag: “hydrolysed collagen peptides” clearly listed.
Yellow flag: vague “collagen blend.”
Red flag: big claims, unclear form.
2. What is the dose per serve?
Many studies use gram-level doses, often around 5–15 g/day depending on the outcome and product. A capsule containing a tiny amount may not match the research dose.

Green flag: clear grams per serve.
Yellow flag: proprietary blend with total dose unclear.
Red flag: fairy-dust dosing hidden behind marketing.
If you’re building collagen into a bigger plan
Collagen is one input. Loading is the instruction. If you’re thinking about connective tissue health as part of staying capable for the long haul, these two pieces are worth reading alongside this one.
If You Can’t Hold 60 Seconds, You’re at Risk →
Lateral chain stability as a baseline — and why it matters for everything downstream.
3. Is there third-party testing?
Especially for marine products, quality control matters. Testing for contaminants, heavy metals and purity is worth looking for.

Green flag: third-party tested, batch tested, transparent quality claims.
Yellow flag: “premium” with no evidence.
Red flag: no testing information.
4. Does it include or recommend vitamin C?
It does not need vitamin C in the same scoop, but collagen synthesis relies on vitamin C-
dependent enzymes. If the product talks about collagen synthesis but ignores cofactors entirely,
that is a sign the marketing may be ahead of the science

Green flag: sensible cofactor discussion.
Yellow flag: vitamin C added but no meaningful dose listed.
Red flag: “rebuilds collagen” with no mention of cofactors or diet.
5. Does the claim match the evidence?
“May support skin hydration” is different from “reverses ageing.”
“May support connective tissue health alongside exercise” is different from “repairs joints.”

Green flag: cautious, specific claims.
Yellow flag: vague beauty/joint language.
Red flag: guaranteed results, dramatic before-and-after claims, or “clinically proven” with no study details.
6. Does it fit the person?
This matters.

Dietary preferences, allergies, cost, medications, medical conditions, pregnancy, surgery, kidney issues, inflammatory conditions, and overall protein intake all matter. So does whether the
person is already doing the basics.
A supplement that makes sense for one person may be unnecessary for another.
Context always wins.
So, Should You Take Collagen?
Maybe.
I know. Deeply satisfying.
But that is the honest answer.
If someone is already eating well, getting enough protein, moving regularly, sleeping reasonably, and doing a sensible loading program for their tendon, joint or bone health, collagen peptides may be a reasonable adjunct to discuss.
If someone is under-eating, sleeping poorly, avoiding load, living on coffee until 2pm, and hoping collagen will do the job of rehab, nutrition and recovery?
No.
That is not a supplement plan.
That is a wish with a scoop.
The better question is not, “Does collagen work?”
The better question is:
“What job are you expecting collagen to do, and have you created the conditions where your body can actually use it?”
For skin, the evidence suggests possible benefit, but funding bias and product variability matter.
For knee osteoarthritis, there is some evidence for symptom improvement, but it should not be treated as a standalone solution.
For tendons and connective tissue, the most convincing model is collagen or gelatin plus vitamin C plus appropriate loading.
For bone, collagen is part of the matrix, but bone health still depends heavily on loading, hormones, mineral status, vitamin D, protein, energy availability and broader health.
That is the grown-up answer.
Less exciting than the ads.
Much more useful.
The Barefoot View: Materials, Workers, Tools and Load
Here is the analogy I’d use in clinic.
A collagen supplement may provide some building materials. But a building site needs more than materials.
It needs workers. It needs tools. It needs instructions.
It needs the right conditions.
And it needs a reason to build.
In the body, the building materials are amino acids and collagen-derived peptides.
The workers are fibroblasts, tenocytes, osteoblasts, chondrocytes and other connective tissue cells.
The tools are vitamin C, iron, copper, zinc, enzymes, oxygen and energy.
The instructions come from local tissue demand, repair signals and mechanical loading.
The conditions include sleep, inflammation, hormones, diet quality, stress, medications and general health.
That is why collagen on its own is incomplete.
Not useless.
Incomplete.

This is where my naturopathic background and osteopathic work overlap nicely. Nutrition
supplies the raw materials and supports the biochemical environment. Movement and loading
tell the body where adaptation is needed.
One without the other is a half-built argument.
And bodies are already complicated enough without adding half-built arguments
Bringing It All Together
Collagen is not nonsense.
But the way collagen is often sold is far too neat.
The body is not a vending machine. You do not insert collagen powder and receive one repaired
tendon, two smoother cheeks, and a knee that now behaves itself on stairs.
You provide materials. The body decides what to do with them.
That decision depends on local tissue demand, mechanical loading, cell behaviour, cofactors,
nutrition, recovery and product quality.
So the useful middle ground is this:
Collagen supplements may support the system, but they do not direct the system.
If you are curious about collagen, start with the bigger question.
- What tissue are you trying to support?
- What load is that tissue receiving?
- Is your diet giving your body enough to work with?
- Are the tools available?
- Is the product actually comparable to what the research studied?
That is where the conversation becomes useful.
Not “does collagen work?”
But “does this make sense for this body, this goal, and this plan?”
If you are dealing with a tendon, joint, or recurring movement issue and want to understand
what your body is actually asking for, book a consultation. We can look at the bigger picture:
your movement, your loading, your history, your recovery, and whether collagen belongs in the
conversation at all.
Experience the Barefoot Difference. Book a consultation:
This information is general in nature and is not a substitute for individual clinical advice. Speak
with your GP, dietitian, pharmacist, or relevant health professional before starting supplements if
you are pregnant, managing a medical condition, taking medication, preparing for surgery, or
unsure whether a product is appropriate for you.
📌 KEY TAKEAWAYS:
- Collagen supplements may provide building materials, but your body decides where they go.
- Loading, nutrition, cofactors and recovery matter as much as the supplement itself.
- Product quality matters. The label “collagen” is not enough information.
- Think adjunct, not standalone fix.
Frequently Asked Questions:
A: Collagen supplements may provide amino acids and small peptides that the body can use as
part of connective tissue turnover. Some studies show benefits for skin hydration, elasticity and
knee osteoarthritis pain, but the evidence varies by product, dose, population and funding
source. They are best viewed as a possible adjunct, not a guaranteed fix.
A: No. Collagen is digested into amino acids and smaller peptides before absorption. Some
collagen-derived peptides can appear in the blood, but the body still decides where materials
are used based on local tissue demand, cell activity, loading, and overall health.
A: Hydrolysed collagen peptides are generally more plausible for absorption than native collagen
because they are already broken into smaller peptide fragments. Some studies show collagen-
derived dipeptides and tripeptides can appear in the bloodstream after ingestion.
A: Vitamin C is important for collagen synthesis because it supports enzymes involved in collagen
formation and stability. You do not necessarily need vitamin C inside the same supplement, but
your overall vitamin C intake needs to be adequate.
A: Collagen may be most biologically plausible when paired with appropriate loading. Research on
gelatin plus vitamin C before exercise suggests this combination may influence collagen
synthesis markers. But tendon and ligament adaptation still depend heavily on progressive
loading, recovery, and individual tissue tolerance.
A: Some research suggests collagen peptides may reduce knee osteoarthritis pain compared with
placebo, but results should be interpreted cautiously. Collagen should not replace strength
work, load management, medical advice, or broader joint health strategies.
A: Yes. Collagen products can differ by source, tissue type, processing method, molecular weight
and peptide profile. That does not automatically make one better for everyone. Product quality,
dose, testing and the evidence behind the specific product matter more than the marketing
category.er joint health strategies.
A: Look for hydrolysed collagen peptides, a clear dose in grams, third-party testing, transparent
sourcing, sensible claims, and ideally some discussion of cofactors such as vitamin C. Be
cautious with products making dramatic claims about reversing ageing, rebuilding joints or
guaranteeing results.
REFERENCES:
Amirrah, I. N., Lokanathan, Y., Zulkiflee, I., Wee, M. F. M. R., Motta, A., & Fauzi, M. B. (2022). A comprehensive review on collagen type I development of biomaterials for tissue engineering: From biosynthesis to bioscaffold. Biomedicines, 10(9), 2307. https://pmc.ncbi.nlm.nih.gov/articles/PMC9496548
Bischof, K., et al. (2024). Impact of collagen peptide supplementation in combination with physical training on musculoskeletal health: A systematic review and meta-analysis. Sports Medicine. https://pubmed.ncbi.nlm.nih.gov/39060741/
Gelse, K., Pöschl, E., & Aigner, T. (2003). Collagens: Structure, function, and biosynthesis. Advanced Drug Delivery Reviews, 55(12), 1531–1546. https://pubmed.ncbi.nlm.nih.gov/14623400
Khatri, M., Naughton, R. J., Clifford, T., Harper, L. D., & Corr, L. (2021). The effects of collagenpeptide supplementation on body composition, collagen synthesis, and recovery from joint injury and exercise: A systematic review. Amino Acids, 53, 1493–1506. https://pmc.ncbi.nlm.nih.gov/articles/PMC8521576
León-López, A., Morales-Peñaloza, A., Martínez-Juárez, V. M., Vargas-Torres, A., Zeugolis, D. I., &Aguirre-Álvarez, G. (2019). Hydrolyzed collagen: Sources and applications. Molecules, 24(22),4031. https://pmc.ncbi.nlm.nih.gov/articles/PMC6891674/
Li, M. C. M., Chow, S. K. H., Wong, R. M. Y., et al. (2021). The role of osteocytes-specific molecular mechanism in regulation of mechanotransduction: A systematic review. Journal of Orthopaedic Translation, 29, 1–9. https://pmc.ncbi.nlm.nih.gov/articles/PMC8138679/
Lin, C. R., Tsai, S. H. L., Huang, K. Y., & Tsai, P. A. (2023). Analgesic efficacy of collagen peptide in knee osteoarthritis: A meta-analysis of randomized controlled trials. Journal of Orthopaedic Surgery and Research, 18, 694. https://pubmed.ncbi.nlm.nih.gov/37717022/
Magnusson, S. P., Langberg, H., & Kjaer, M. (2010). The pathogenesis of tendinopathy: Balancing the response to loading. Nature Reviews Rheumatology, 6(5), 262–268. https://pubmed.ncbi.nlm.nih.gov/20308995
Myung, S. K., & Park, K. (2025). Effects of collagen supplements on skin aging: A systematic review and meta-analysis. The American Journal of Medicine. https://pubmed.ncbi.nlm.nih.gov/40324552/
Nakamichi, R., et al. (2024). The role of mechanotransduction in tendon. Journal of Orthopaedic Research. https://pmc.ncbi.nlm.nih.gov/articles/PMC11301520/
Pinnell, S. R. (1985). Regulation of collagen biosynthesis by ascorbic acid: A review. Yale Journal of Biology and Medicine, 58(6), 553–559. https://pmc.ncbi.nlm.nih.gov/articles/PMC2589959/
Pu, S. Y., et al. (2023). Effects of oral collagen for skin anti-aging: A systematic review and meta- analysis. Nutrients, 15(9), 2080. https://pmc.ncbi.nlm.nih.gov/articles/PMC10180699/
Sato, K., et al. (2020). Collagen-derived di-peptide, prolylhydroxyproline (Pro-Hyp): A new low molecular weight growth-initiating factor for specific fibroblasts associated with wound healing. Frontiers in Cell and Developmental Biology, 8, 548975. https://pmc.ncbi.nlm.nih.gov/articles/PMC7728856
Shaw, G., Lee-Barthel, A., Ross, M. L. R., Wang, B., & Baar, K. (2017). Vitamin C-enriched gelatin supplementation before intermittent activity augments collagen synthesis. The American Journal of Clinical Nutrition, 105(1), 136–143. https://pubmed.ncbi.nlm.nih.gov/27852613/
Virgilio, N., et al. (2024). Absorption of bioactive peptides following collagen hydrolysate ingestion. Frontiers in Nutrition, 11, 1416643. https://pmc.ncbi.nlm.nih.gov/articles/PMC11325589
Wauquier, F., et al. (2019). Human enriched serum following hydrolysed collagen absorption modulates bone cell activity: From bedside to bench and vice versa. Nutrients, 11(6), 1249. https://pmc.ncbi.nlm.nih.gov/articles/PMC6627680






